The Intracept Procedure
The Intracept procedure, also called basivertebral nerve ablation, treats a specific cause of chronic low back pain that standard treatments often miss: pain coming from the vertebrae themselves. It is a minimally invasive, one-time outpatient procedure offered by Dr. Carrera's team in Castle Rock, Colorado.
The Kind of Back Pain Intracept Treats
Low back pain does not always come from the discs or the spinal joints. In some people, the source is the bone at the top and bottom of each vertebra, right where bone meets disc. These surfaces are called endplates. As a disc wears down, the endplates next to it can become damaged and inflamed, and they begin sending steady pain signals through a small nerve that runs inside the bone, called the basivertebral nerve.
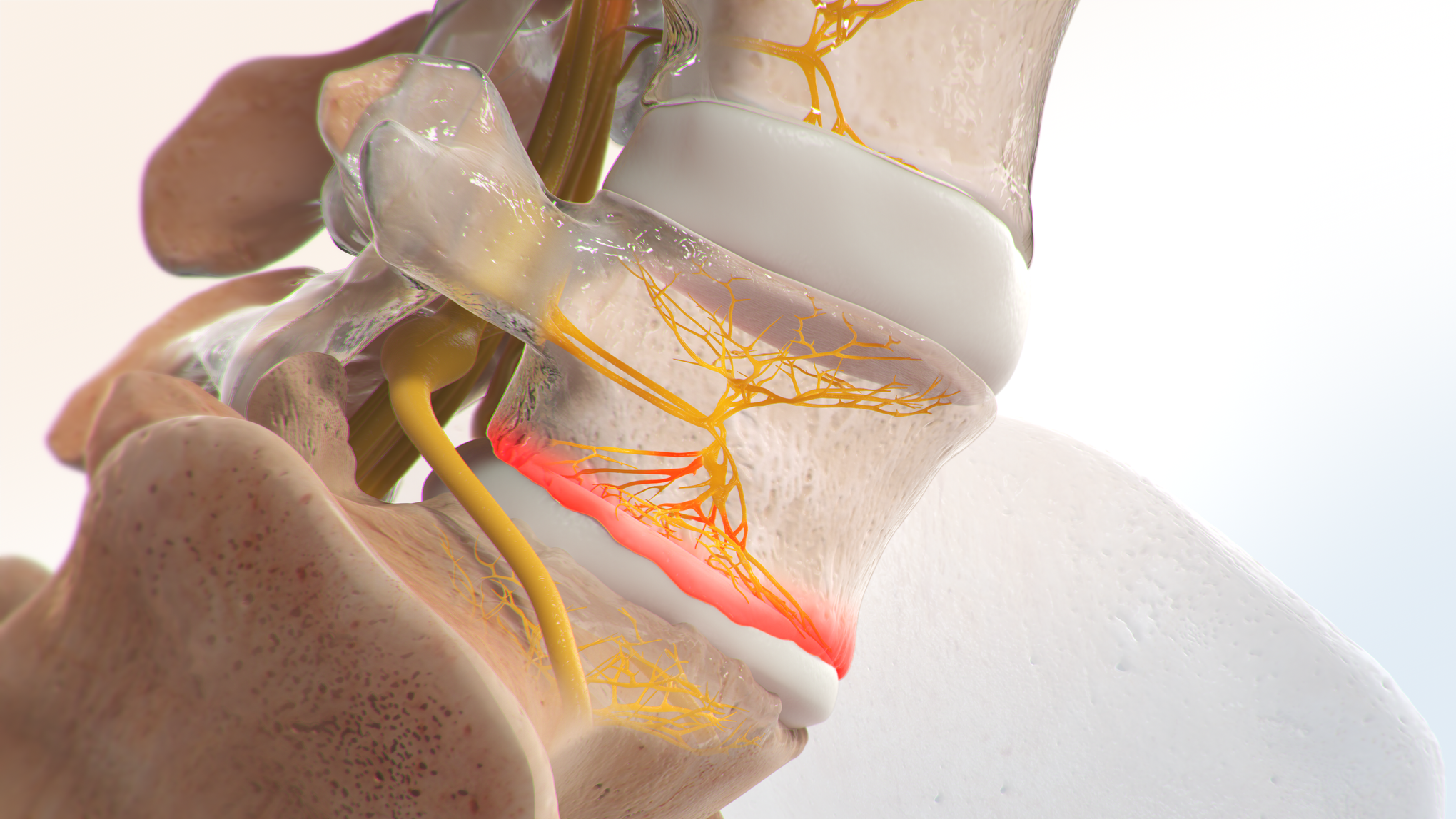
This type of pain has a recognizable pattern. It is usually a deep, aching pain in the middle of the low back that gets worse with bending forward, sitting for long periods, or physical activity. If that sounds familiar and other treatments have not given lasting relief, the vertebrae may be the piece of the puzzle nobody has looked at.
How the Procedure Works
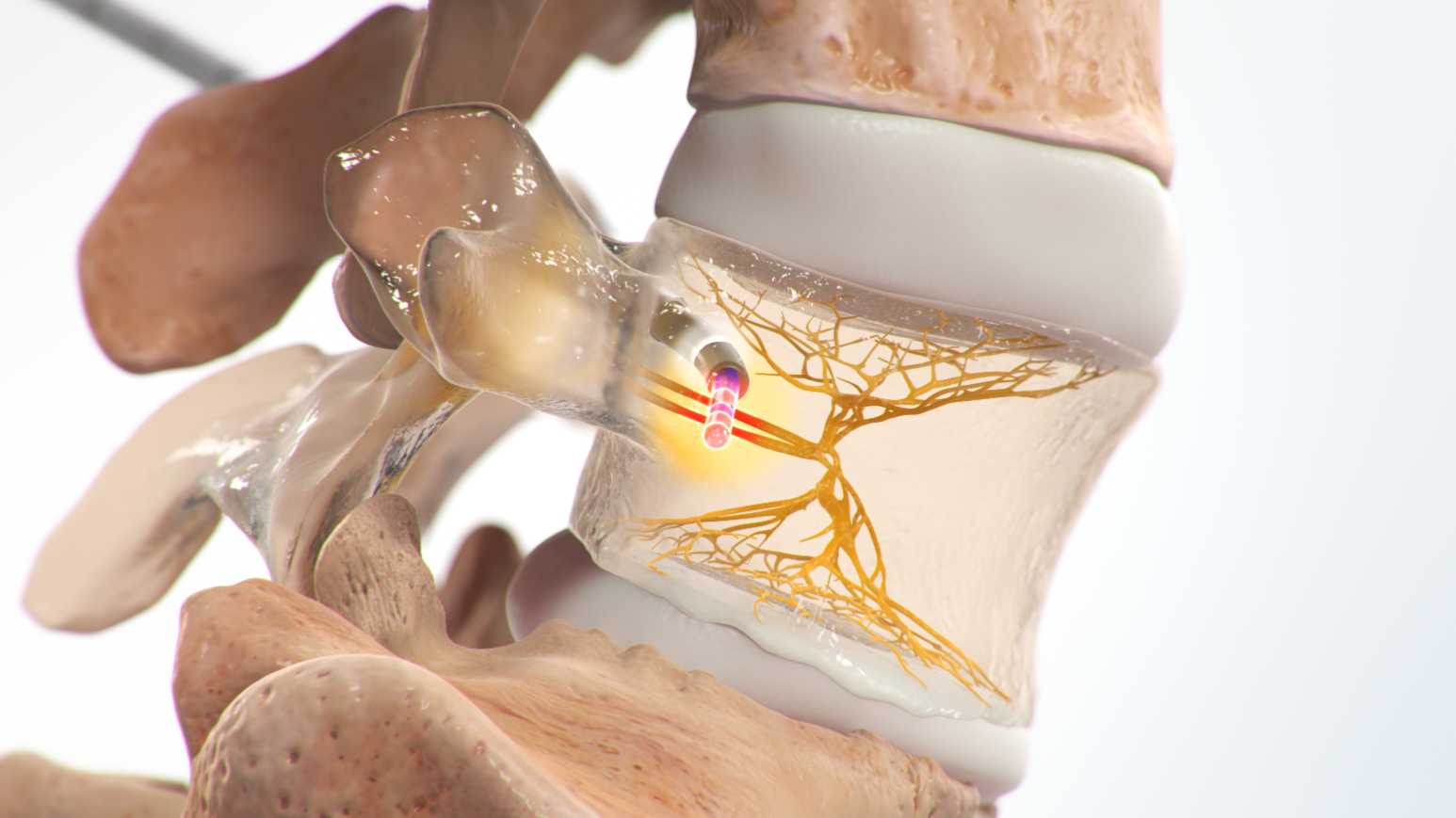
Intracept is done through a small incision in the lower back. Using X-ray guidance, a narrow channel is created into the vertebra, and a probe delivers radiofrequency energy to heat the basivertebral nerve. Once treated, the nerve stops carrying pain signals from the endplates. Nothing is implanted, and the structure of the spine is not changed. You receive anesthesia so you are comfortable during the procedure, and you go home the same day.
Why it is designed to be a one-time treatment. The nerves treated in facet joint ablation grow back over time, which is why that procedure is repeated every year or two. The basivertebral nerve does not grow back the same way. That is why Intracept is intended as a single treatment with lasting relief rather than something done on a schedule.
Who Is a Good Candidate
Intracept fits a specific group of patients. In general, candidates have had low back pain for at least six months, have tried other care such as physical therapy, medications, or injections without lasting relief, and have specific changes at the endplates that show up on an MRI. The MRI finding is the deciding factor. It is how we confirm the pain is truly coming from the vertebrae and not from somewhere else. Reviewing your imaging is the first step, and if you do not have a recent MRI, we can arrange one.
Who It Is Not For
Intracept does not treat every kind of back pain. Pain that mainly comes from a herniated disc, a pinched nerve, the SI joint, or the facet joints calls for different treatment, and each of those problems has its own effective options. Leg pain is usually a clue that the source is somewhere other than the vertebrae. A careful evaluation sorts this out before any procedure is considered.
What to Expect Afterward
Most people have some soreness at the incision site for a few days and return to their usual routine within about a week. Relief does not always arrive overnight. Some patients notice improvement within the first few weeks, and for others it builds over the first two to three months as the nerve quiets down.
Common Questions
Does the nerve grow back? No. Unlike the nerves treated in facet ablation, the basivertebral nerve is not expected to regrow. That is why Intracept is designed as a one-time treatment.
Is this the same as the ablation used for facet joint pain? Both use radiofrequency energy, but they treat different nerves for different problems. Facet ablation treats the small joints at the back of the spine and is repeated as those nerves recover. Intracept treats the nerve inside the vertebra itself.
Will insurance cover it? Coverage varies by plan. Our team checks your benefits and handles the authorization process before anything is scheduled, so you know where you stand.
The Intracept Procedure in Castle Rock
Dr. Carrera is double board-certified in interventional pain medicine and physical medicine and rehabilitation. He evaluates and treats chronic low back pain for patients from Castle Rock, Castle Pines, Lone Tree, Parker, Highlands Ranch, Centennial, Denver, Monument, and Colorado Springs, and surrounding communities.
Wondering if your chronic low back pain could be coming from the vertebrae themselves? Call 720-455-3775 to find out if you are a candidate for the Intracept procedure.
Written by Eduardo Carrera, MD Double board-certified in Interventional Pain Medicine and Physical Medicine & Rehabilitation
Dr. Carrera completed his entire medical training at the University of Colorado — medical school, PM&R residency, and pain management fellowship — and serves as an oral examiner for the American Board of Physical Medicine and Rehabilitation. He practices in Castle Rock, Colorado, where he treats spine, joint, and nerve pain using diagnostic injections, nerve ablation, and other non-opioid procedures. More about Dr. Carrera →